
The right to die: Would Nevada bill endanger society’s most vulnerable?










Lynda Brooks-Bracey is not ready to take lethal pills to end her life.
The 57-year-old Las Vegan continues to endure exhausting chemotherapy that won’t cure her terminal pancreatic cancer but buys her more time. Still, she wants to know that in the end, she can shorten the suffering of her death if she wishes.
“I am a strong believer in the circle of life, a believer in God … but I don’t think I or my family should have to see me suffer,” Brooks-Bracey, who witnessed her first husband die of leukemia, told Nevada legislators in March.
Through her advocacy, Brooks-Bracey has become one of the faces in Nevada’s debate over what proponents refer to as medical aid in dying and what opponents call assisted suicide.
On Wednesday, the Nevada Senate in an 11 to 10 vote approved Senate Bill 239, which allows medical providers to prescribe lethal medication to terminally ill patients that they can self administer. The bill now goes to the Nevada Assembly for further consideration.
In an interview this month, Brooks-Bracey’s smiling composure cracked when she spoke of wanting to set an example for her four children of fighting for what she believes in, even in death.
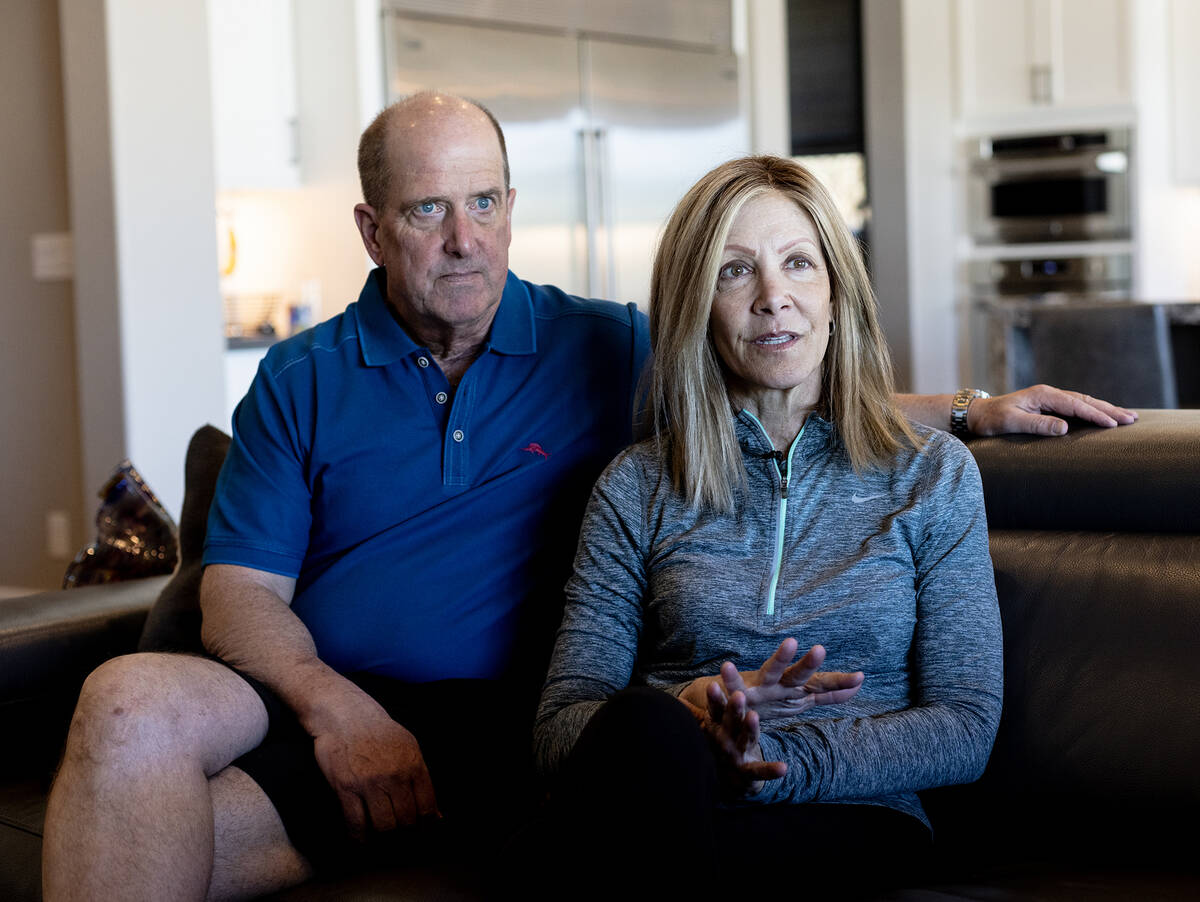
“When this subject comes up, a lot of people feel very involved in my choice,” she said from the living room of her elegant home on the edge of Red Rock Canyon, her physician husband at her side.
“And I always say, I’m totally fine if it’s not their choice … I would be the person at their bedside holding their hand because everyone should have the choice of how they choose to pass away.”
Opponents of the legislation argue, however, that more vulnerable members of society — the poor, the disabled, those without loving family members — could be pressured into making such a choice, should the measure become law.
One such opponent is Reno resident Brianna Hammon, who has cerebral palsy and serves as an advocate for disabled people. Hammon, who has testified against similar bills in previous legislative sessions, is another face in the state’s debate.
Hers was not a face seen, however, during March’s legislative hearing. The Legislature did not provide public notice of the hearing until just hours beforehand, providing insufficient time for disabled opponents in particular to attend and make their views known, opponents said.
Hammon, who uses a wheelchair, and her mother, Deidre, also an activist, said disabled people already are marginalized and struggle to make their voices heard.
“Well-meaning doctors look at me and think I would be better off dead. They will think it’s a favor to offer to suicide me,” said Brianna, who used a voice device to deliver prepared comments to the Review-Journal during a Zoom meeting.
“After death becomes a medical option, it will be hard to get good drugs,” she said. “If I go to the emergency room or urgent care, doctors will assume that I am terminal. They do it now.”
Potential for abuse
Senate Bill 239 authorizes patients to request that a medical practitioner prescribe medication designed to end their life. A patient must be at least 18 years old and have been diagnosed by two practitioners with a terminal condition, meaning a life expectancy of possibly six months or less.
SB 239 states that the patient needs to be mentally capable of making such a decision and “is not requesting the medication because of coercion, deception or undue influence.”
In the U.S. 10 states and the District of Columbia have authorized medical aid in dying, including Nevada’s neighbors California and Oregon, Oregon being the first.
The Nevada bill is modeled after Oregon’s Death with Dignity Act, which “has been in practice for more than 25 years without a single instance of abuse or coercion,” according to advocacy group Compassion & Choices.
Bill opponents are skeptical of the claim. “One of the major flaws is that we don’t know how it’s working because health care privacy laws prevent us from questioning anything,” Reno internist Dr. Kirk Bronander said during the March legislative committee meeting.
“The prescribing doctors are unknown, the circumstances and the patient’s names are completely unknown,” Bronander said before he was cut off by Sen. Fabian Donate, chairman of the Senate committee holding the hearing, who was enforcing a legislative rule limiting committee testimony to two minutes.
This month, Bronander continued the thought in an interview with the Review-Journal. “There’s never been a case documented of coercion because we just don’t know,” he said. “The patient is dead, and the person who would have coerced the patient isn’t telling anybody.”
Both the Oregon law and the Nevada legislation require that the patient’s underlying disease be put as a cause of death, without referencing the lethal pills, obscuring transparency.
There is anecdotal evidence of at least the potential for abuse.
Dr. Brian Callister, Bronander’s medical partner, said that twice when transferring patients out of state, one to Oregon and one to California, the medical director for state insurance told him they would not provide proven treatments that potentially could cure the patients. But they asked if he had considered medically assisted suicide, he said in a video on the website of Patients Rights Action Fund.
“It’s a lot cheaper to grab a couple of drugs than it is to provide life-sustaining therapy,” he said on the video.
In an interview, Callister said that medical privacy laws prevented him from providing more details on the patients. He said that in one of the instances, the patient’s family favored what he describes as assisted suicide, though the patient did not. He did not know the patients’ outcomes, the patients having left his care when they left the state.
The Nevada bill states, “It is important that patients have the full range of options for their care, especially at the end of their lives.”
Yet the bill does not require insurance companies to provide life-sustaining therapies recommended by a patient’s physician.
Quality of life top concern
Senate Bill 239 states, “Patients with a terminal illness may undergo unremitting pain, agonizing discomfort and a sudden, continuing and irreversible reduction in their quality of life. … ”
Medical aid in dying “provides an additional palliative care option for persons with a terminal illness who seek to retain their autonomy and some level of control over the progression of their disease or ease unnecessary pain and suffering.”
Data from Oregon indicates that quality of life was of greater concern than pain to those who have opted for medically assisted dying in that state.
In 2022, as in the previous years, the most frequently stated end of life concerns were “decreasing ability to participate in activities that made life enjoyable (89 percent), loss of autonomy (86 percent) and loss of dignity (62 percent),” according to an Oregon annual report.
Burden on family, friends/caregivers ranked fourth (46 percent), followed by losing control of bodily function (45 percent). “Inadequate pain control, or concern about it ” came next (31 percent), followed by financial implications of treatment (6.1 percent).
The pain of a dying patient can be treated through the use of medications, said Las Vegas hospice physician Dr. Catrisha Cabanilla-Del Mundo. To alleviate pain in some cases, the amount of mediation must be increased to the point that the patient is sedated and no longer can provide a purposeful response.
The decision to increase medication to such levels is one made with the patient and the patient’s family, said Cabanilla-Del Mundo, who works for Nathan Adelson Hospice.The approach is not intended to end the patient’s life but to ease suffering, she said.
A hospice multidisciplinary team includes a doctor, nurse, social worker and counselor to address all forms of pain: emotional, spiritual, interpersonal, spiritual or existential.
“And I can even argue that physical suffering – the physical pain – is probably the easiest pain to treat, because we have medicine and we can objectively see the change in the patient’s perception of pain,” she said. “But other things that cause pain, which are more intangible … those are more difficult.”
Cabanilla-Del Mundo said she personally would not be comfortable prescribing drugs to end a patient’s life. She said she hoped that under a right-to-die measure, a multidisciplinary team would work with patients to relieve their suffering and that lethal medication would be considered only as a last resort.
As the bill is currently written, a multidisciplinary approach is not required.
Poll shows widespread support
In the Nevada Senate on Wednesday, two senators spoke on Senate Bill 239 before a vote was taken. There was no debate.
Democratic Sen. Edgar Flores, one of the bill’s primary sponsors, first gave a general overview of the bill. Republican Sen. Jeff Stone then spoke in opposition, saying the measure threatens “our most vulnerable populations.”
Stone noted the opposition of Catholic bishops in Las Vegas and Reno. and of the American Medical Association, which says “physician assisted suicide is fundamentally inconsistent with a physician’s professional role,” he said.
However, a new poll shows that medically aided dying has gained widespread support among Nevadans.
A record 82 percent of Nevada voters polled supported legislation giving terminally ill Nevadans the option of medical aid in dying, according to the poll released on Wednesday by Compassion & Choice before the Senate vote.
The poll by Susquehanna Polling & Research surveyed 600 registered Nevada voters. The measure was popular across party lines, religious faiths, ethnicities and counties.
“I pray this poll spurs our Nevada lawmakers to pass a medical aid-in-dying law this year, in time for seriously ill Nevadans like me who desperately need this option,” Brooks-Bracey, the Las Vegan with terminal pancreatic cancer, said in a Compassion & Choices new release.
“If their constituents’ overwhelming support for medical aid in dying doesn’t persuade lawmakers to pass this compassionate legislation, I don’t know what will.”
Canada’s expanding law
In Canada, where medical aid in dying has been the law since 2016, more than 31,000 people have died in this manner, accounting for more than 3 percent of all deaths, according to the Toronto Star.
As the numbers in Canada have risen, so have concerns about the potential for abuse. News media reports tell of individuals opting for, or considering, medical aid in dying when they couldn’t find affordable housing or after falling into poverty.
Canada was poised to expand in March the medical aid in dying option to those who suffer a mental illness as the sole qualifying condition. After a public outcry, the government delayed the expansion.
Opponents in Nevada fear a similar slippery slope.
“With all the difficulties and potential abuses around this, it’s just not something we should be supporting as a society,” Bronander said.
For those near death, he said, we should “support them and hold their hand.”
Contact Mary Hynes at mhynes @reviewjournal.com or 702-383-0336. Follow @MaryHynes1 on Twitter.














